Conquer Your Acne through Isotretinoin IPledge

Don’t neglect any skin problems.
Any skin bump or blister you might have, Dr.Paul usually starts with the following questions:
●How long has the eruption or lesion been present?
●How did it look when it first appeared, and how is it now different?
●Where did it first appear, and where is it now?
●What treatments have been used, and what was the response, this time and previously?
●What associated symptoms, such as itching or pain, are associated with the lesion?
●Are any other family members affected or have a similar history?
●Has the patient ever had this rash or lesion before? If so, what treatment was used, and what was the response?
●What does the patient think caused the rash or lesion?
●Is anything new or different (eg, medications, personal care products, occupational or recreational exposures)?
Additional questions that may be helpful include:
●Does the patient have any chronic medical conditions?
●What medications does the patient take currently, what have they recently taken, including over-the-counter and herbal therapies?
●Has there been any increase in stress in their life?
●What is the social history, including occupation, hobbies, travel?
●Does the patient have any underlying disease or allergies?
●Does the patient have pets?
●Does the patient have risk factors for sexually transmitted diseases?
PHYSICAL EXAMINATION — The physical examination of a skin complaint, which includes visual inspection and palpation of the skin and sometimes additional examination aided by a Wood’s lamp or a dermatoscope, is aimed at assessing the following:

A Full Skin Examination is done after taking history of the problem.
●Type of lesion
●Morphology of individual lesions
●Configuration of multiple lesions (eg, scattered, grouped, linear, etc)
●Distribution of lesions
●Color
●Consistency and feel

The initial approach to the patient presenting with a skin problem requires a detailed history of the current skin complaint and a complete skin examination. In many cases, the patient’s general medical history may be relevant to the diagnosis of skin disorders.
●Key questions for the patient include the time of onset, duration, location, evolution, and symptoms of the rash or lesion. Additional information on family history, occupational exposures, comorbidities, medications, and social or psychological factors may be helpful.
●The type, shape, arrangement, and distribution of the lesions are cardinal features to be identified by visual inspection and palpation.

●Secondary changes are due to spontaneous evolution, manipulation, superimposed infection, or previous treatment and may alter the morphology of the primary lesion.
●The lesion location often provides a clue to diagnosis, since many skin disorders have a predilection for particular body sites
PRIMARY SKIN PROBLEMS – CLASSIFICATION
Primary lesions are either the first visible lesion or involve the initial skin changes. The terms used to describe primary skin lesions include the following:
●Macules are nonpalpable lesions ≤1 cm that vary in pigmentation from the surrounding skin. Patches are nonpalpable lesions >1 cm. There are no elevations or depressions.
●Papules are palpable, discrete lesions measuring ≤5 mm in diameter. They may be isolated or grouped.
●Plaques are large (>5 mm) superficial slightly raised lesions, often formed by a confluence of papules.
●Nodules are palpable, discrete lesions measuring ≥5 mm in diameter; tumors are large nodules. They may be isolated or grouped and may or may not present with surface changes.
●Telangiectasia is a dilated superficial blood vessel.
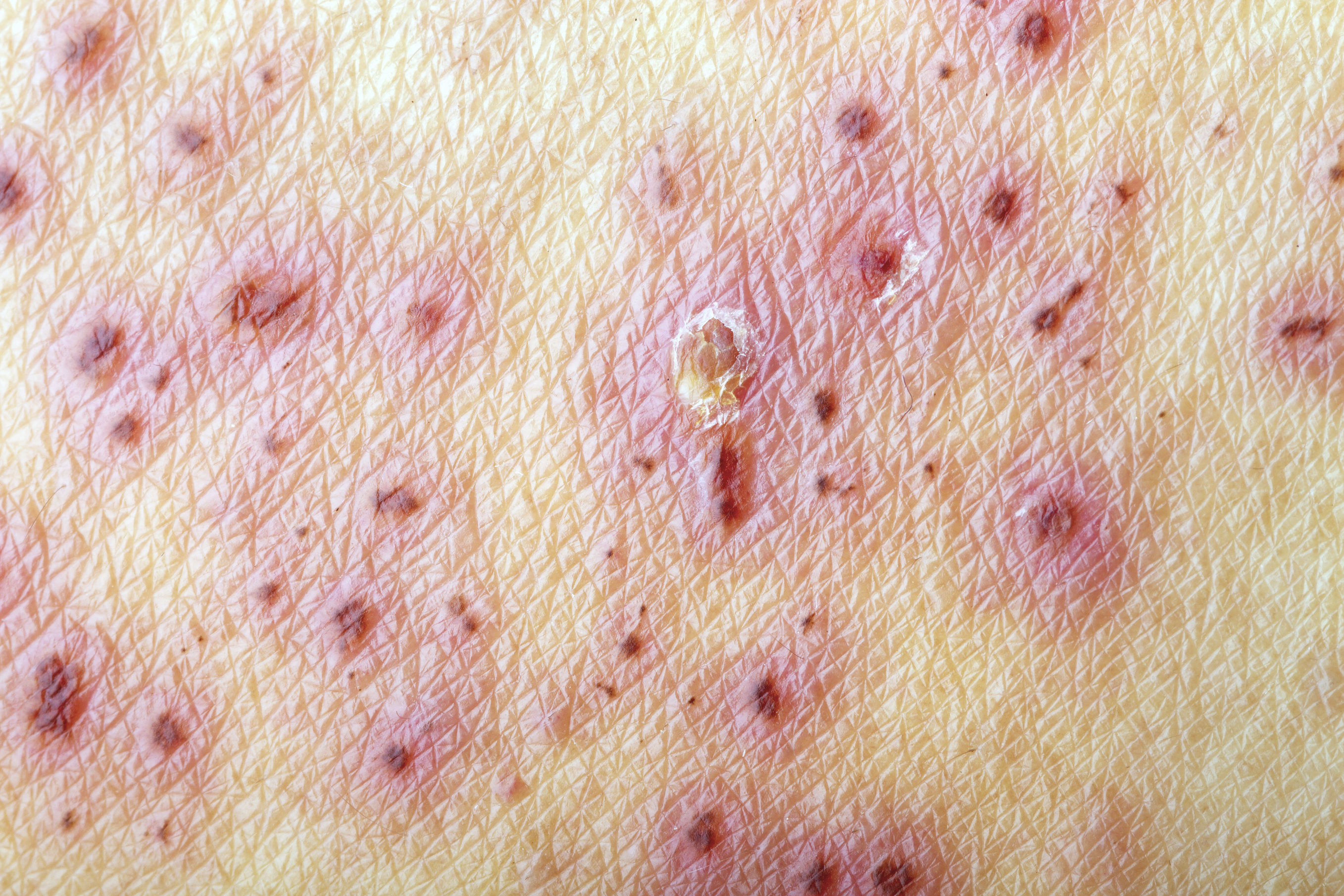
●Purpura are red-purple lesions that do not blanch under pressure, resulting from the extravasation of blood from cutaneous vessels into the skin. Purpuric lesions can be macular or raised (palpable purpura)
●Pustules are small, circumscribed skin papules containing purulent material.
●Vesicles are small (<5 mm diameter), circumscribed skin papules containing serous material. Bullae are large (≥5 mm) vesicles.
●Wheals are irregularly elevated edematous skin areas that are often erythematous. The borders of a wheal are sharp but not stable; they may move to adjacent uninvolved areas over periods of hours.
SECONDARY SKIN PROBLEMS – CLASSIFICATION
Secondary lesions — Secondary lesions of the skin represent evolved changes from the skin disorder, due to secondary manipulation or as a result of infection. Examples include:
●Excoriation describes superficial, often linear skin erosion caused by scratching.
●Lichenification is increased skin markings and thickening with induration secondary to chronic inflammation caused by scratching or other irritation.
●Edema is swelling due to accumulation of water in tissue.
●Scale describes superficial epidermal cells that are dead and cast off from the skin.
●Crust is dried exudate, a “scab”.
●Fissure is a deep skin split extending into the dermis.
●Erosion is a superficial, focal loss of part of the epidermis. Ulceration is focal loss of the epidermis extending into the dermis. Lesions may heal with scarring.
●Atrophy is decreased skin thickness due to skin thinning.
●Scar is abnormal fibrous tissue that replaces normal tissue after skin injury.
●Hyperpigmentation is increased skin pigment; hypopigmentation is decreased skin pigment; and depigmentation is total loss of skin pigment.

For any kind of skin problem, first consult Dr.Paul Kattupalli in our clinic.
